Snoring Remedies? Introduction and Positional Therapy Results
Snoring occurs when the tissues of the airways relax during sleep causing the air to vibrate as it passes over them, in a similar way that deflating a balloon causes the balloon's neck to vibrate and make that familiar raspberry sound.
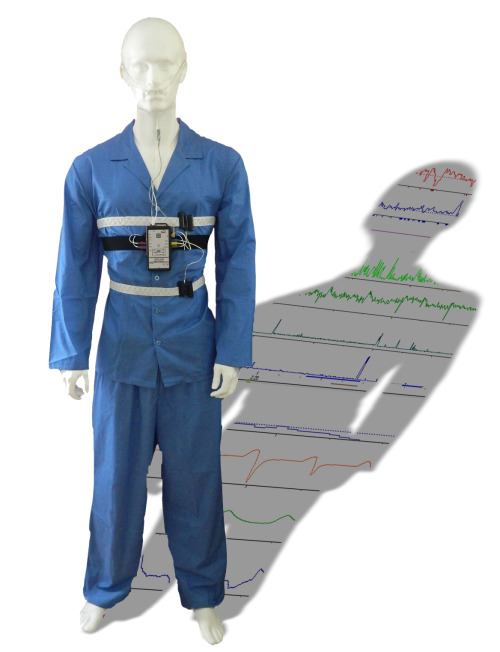
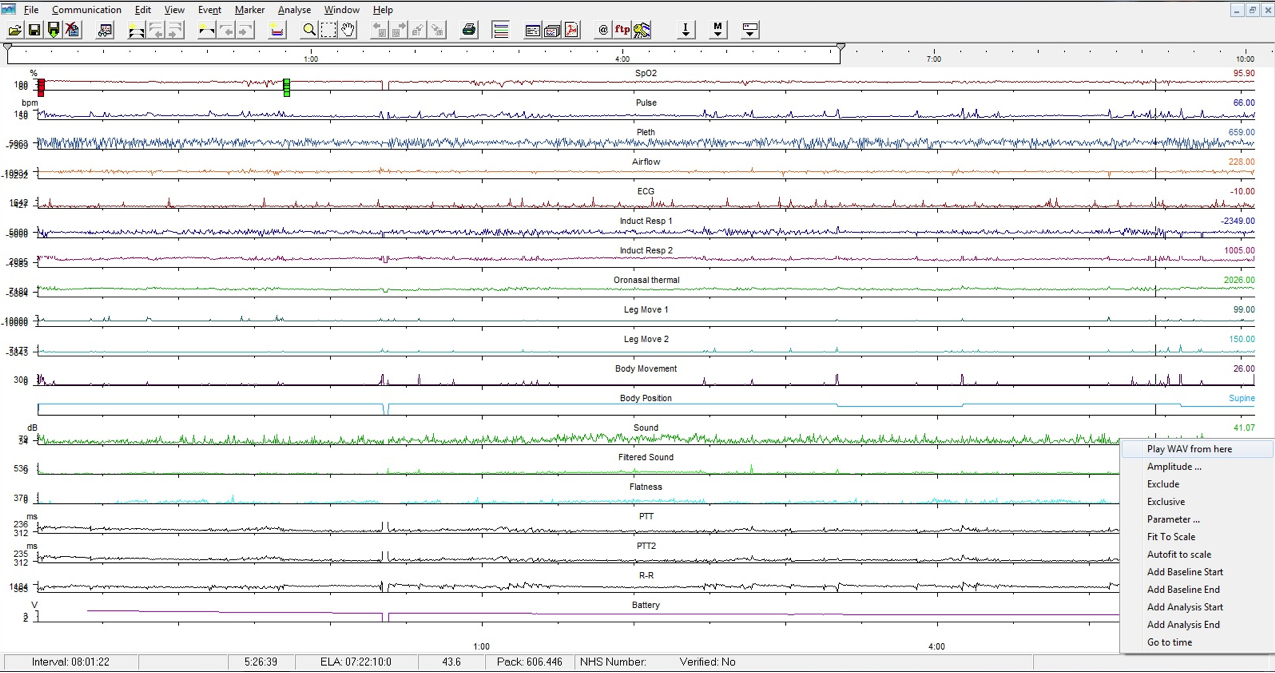
This can be illustrated by the following airflow waveform taken from my snoring using Stowood's Black Shadow Sleep Monitor.
What should have been nice smooth breaths like these...

...ended up becoming jagged saw-toothed breaths like these...

...resulting in a rasping snore.
To give you an idea of what the Visi-Download software allows me to see (and how the vibrations above actually sound) I've made a short video of a few snores that I recorded on one of my baseline nights:
Snoring can simply be just that - a noise, it can be a nuisance if it's too loud as it can wake others in the house, if it's loud enough it can actually wake the sleeper! However, it can also be much more than just a noise. Besides being the cause of much nocturnal anger and maybe even the cause of a relationship breakdown, it can also be a sign of a greater health issue such as sleep apnoea.
I snore. In fact my snoring is sometimes so loud that I hear it in my dreams.
If only that were as as serious as it got, but my snoring is actually due to sleep apnoea. As documented in many posts on this blog, I have mild sleep apnoea.
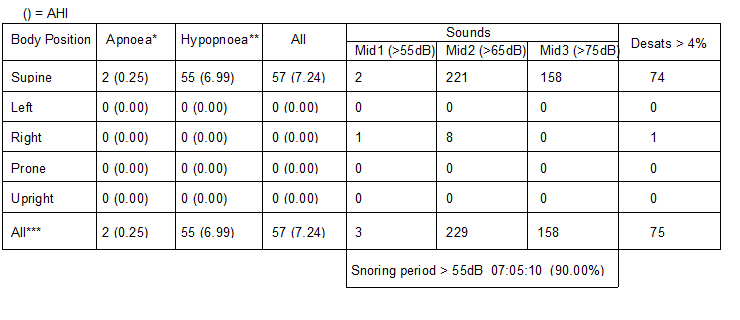
I've found some ways to bring the apnoea to acceptable levels with a typical AHI of between 1 and 3, (an AHI of under 5 is considered normal if it doesn't cause symptoms such as daytime tiredness etc). The way that I did this was to keep off my back when I slept by using a Rematee belt. This also had a knock-on effect of reducing my snoring, but not eliminating it.
On the nights that I've recorded while using the Rematee to keep me off my back, my AHI has been stable and my snoring has reduced (the residual respiratory events are mainly hypopneas, although the lowest that my oxygen saturations drop to has improved, it still drops to around 79%).
Besides looking for other ways to bring my AHI down even more, I want to go further and eliminate my snoring. I guess that my long term quest is to see if it's possible to have the much hyped perfect night's sleep.
Many snoring remedies (and there are many) say that they are not suitable for snoring that is caused by sleep apnoea, so with my new found side-sleeping "normal" AHI and some residual snoring I now find myself in a good position to put them to the test.
Quantifying Snoring
The problem is that snoring is hard to quantify. Yes, you could ask a partner, but that answer would be fairly subjective. You could judge by how you felt in the morning, but again that is subjective. You could even place a Dictaphone beside the bed to record your snoring but besides but again, how do you score the recording?
One of the channels that Stowood's Black Shadow sleep monitor measures is snoring, and it does this via a calibrated microphone, allowing you to quantify how loud each snore actually is. It also derives a second channel from the sound to identify individual snores, thereby allowing you to actually have a snore-count. From there it calculates a snore-index (a number of snores per hour, grouped according to volume).
So, my method is this:
By keeping off my back I am essentially apnoea-free, leaving only the snoring to be addressed, so to ensure this and to eliminate the effects of a variable sleep position on my snoring (and to bring my AHI to normal), I'll be wearing the Rematee belt whilst putting a different snoring remedy to the test each night hoping to eliminate my remaining snoring.
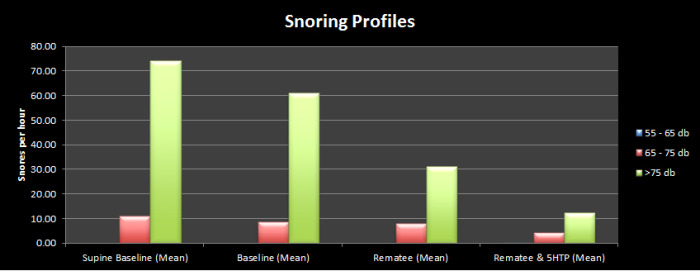
I'll record sleep data for three nights per selected remedy and calculate the mean snoring profile for each by graphing each remedy according to:
- Hourly snores between 55db and 65db
- Hourly snores between 65db and 75db
- Hourly snores greater than 75db
This "Snore Profile" will not only allow me to see if the total snores have been reduced, but it will allow me to see if the remaining snores are quieter.
This graph shows the mean snore profile for my Supine Baseline, Free-to-Move Baseline (calculated from the same nights), and my Rematee baseline.
;)
The majority of my snores are louder than 75db regardless of whether I sleep on my side, back or am free to move around! Not unexpectedly then, it follows that the next largest chunk of my snoring falls between 65 and 75 db with hardly any under 65db.
The "Remedies"
There are plenty of "remedies" available. Some of these are traditional remedies (using the term loosely), and some are more modern commercially available remedies.
- Positional Therapy - (Tennis Ball / Rematee) already shown above
It's clear to see the positive effect that side-sleeping has on reducing my snoring. It reduces my snoring by over 50%, so it is likely that this in itself will be a clear leader in the remedy league table. I suspect that for many snorers (where their snoring is not caused by apnoea) that the Rematee and side-sleeping could eliminate snoring completely.
- Mandibular Advancement Devices
- Nasal dilation
- Snore Spray
- Humidifier by the bedside
- Anti-Snore Ring (Acupressure)
- Anti Snore strip (on roof of mouth)
- Drinking a glass of water before bed
- A night time garlic gargle
- Toothpaste under the nose
- Electric snore-shocker devices
- Nasal irrigation
I also want to explore the following to see if they have an effect on my snoring.
- 5-HTP
- Melatonin
- L-Tryptophan
- Blood sugar levels
- Large dose of vitamin B6
I'll pick from this list (avoiding some completely) and put them to the test for three nights to get a mean snoring value. To avoid creating a very long post I intend to create a separate post introducing each remedy (and how well it performed). When I've finished I'll then chart the results together.
Besides bringing my AHI to an acceptable level to address the residual snoring, part of the reason for staying on my side for the entire night is that it will allow a fair comparison of snoring in all sleep stages (I typically spend around 2h10 minutes in REM and 45 minutes in Slow Wave Sleep). I'll also be keeping an eye on my Zeo stats to see if any of the methods have an effect on my sleep composition. I expect that the methods that rely on disturbing you during snoring episodes may have a negative effect on REM or Slow Wave Sleep.
 Hypnagogia Blog
Hypnagogia Blog
5-HTP Results
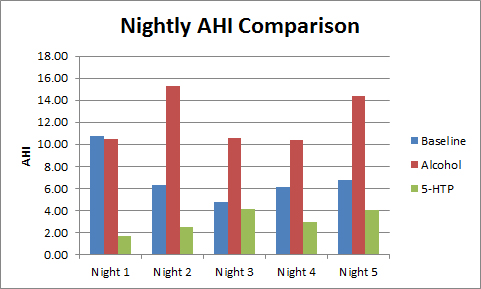
Using the method detailed in this post I decided to see if 5-HTP had any effect on my snoring.
I was keen to try out 200mg of 5-HTP first, given that it had previously had such a positive effect on my AHI.
My thinking was that if 5-HTP had been able to reduce the gross movements of my airways that are responsible for obstructive sleep apnoea, then maybe it would also be able to reduce the smaller movements that are responsible for snoring. However, I suspected that as it hadn't been able to completely prevent airway restrictions that it wouldn't have an effect on the smaller movements.
It seems that I was wrong. The results were promising to say the least.
5-HTP was able to reduce my snoring further than that offered by just sleeping on my side.
Given that from my data alone there are two indications that 5-HTP is beneficial to sleep (AHI reduction and a reduction in snoring) I would love to see a larger scale experiment or trial take place, after all I am just "n=1".
Prior to taking 5-HTP I researched it in medical literature with regards to dosage and possible side-effects. After seeing my results I went back to the literature and started looking for a possible mechanism or explanation as to why 5-HTP might have this effect.
I'm working on a summary of what I've found and will post it in the near future.
For the future:
- I'm curious as to whether the 5-HTP would reduce my supine snoring index, given that my snoring is at its loudest and most frequent when on my back so I will record a three-night mean of 5-HTP sleep when I will be free to move and produce supine and free-to-move snoring indexes via the Visi-Download software.
- I'm also curious to see what different doses would achieve, so I'll carry out three night mean trials of side-sleep + 50mg, 100mg and 300mg of 5-HTP and measure the effect on my AHI, snoring profile and sleep stage data.
Experiment, Explanations, Substances 

;)
;)
;)
;)
;)
;)
;)
;)
;)
;)
;)
;)
;)
;){kind=link}
;){kind=link}